When faced with a red or white lesion or a non-healing ulcer that raises suspicion of malignancy, the biopsy you perform is often the most decisive step in diagnosis and patient care.
During the Biopsy Masterclass on Oral and Maxillofacial Diagnosis, Dr. Sujata Mohanty shared key clinical pearls that every dentist and oral physician should keep in mind.
The Traditional Teaching — Biopsy at the Margin
Many of us were trained to biopsy at the margin of a lesion, capturing both abnormal and adjacent normal mucosa.
The idea was to highlight the transition zone for diagnosis.
But here’s the catch — for suspected malignancy, this approach may actually be harmful except for verrucous lesions.
How Much Tissue Is Enough?
For accurate pathology, specimen size matters. A biopsy should measure at least 1–1.2 cm in length.
This leads to three simple rules of thumb for non-verrucous lesions:
- Small lesions: Perform an excisional biopsy with a 3–4 mm margin.
- Larger lesions over 1 cm in length in at least one dimension: Take an incisional biopsy of the representative part, 3-4 mm in depth and ≥1 cm in length, staying entirely within the lesion.
- Much larger lesions: Multiple biopsies may be needed — but again, none should extend into normal tissue.
- In case of verrucous lesions, considering that the risk of their seeding is very low and that the diagnosis may depend on the comparison of the pushing border of the lesion with the normal tissue, it is acceptable to include peripheral normal tissue.
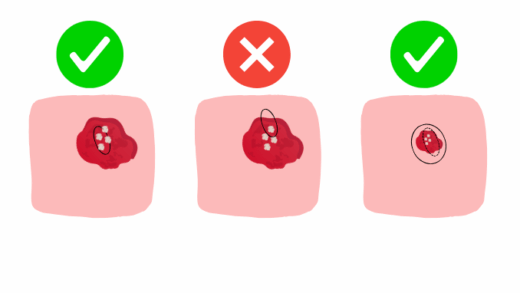
Visual Guide: Correct vs. Incorrect Biopsy Technique
Figure: Correct and incorrect oral biopsy technique for suspected malignant non- verrucous oral lesions
Left: Correct incisional biopsy (1 cm length) within the lesion.
Middle: Incorrect biopsy extending into normal tissue (not recommended).
Right: Excisional biopsy of a small lesion with a 3–4 mm margin.
Don’t Forget Documentation
When excising small lesions, it is critical to document the site:
- Take photographs.
- Record the location relative to anatomical landmarks.
If the lesion is later diagnosed as malignant, the surgeon will need to plan a wide excision, and without precise records, locating the original site after healing may be difficult.
Clinical Takeaway
Biopsy of potentially malignant oral disorders and other suspected malignant lesions is not just about removing tissue — it’s about doing it thoughtfully to protect both diagnosis and prognosis.
Take the most representative part of the lesion, at least 1–1.2 cm in length, without extending into normal tissue.